Electroshock Therapy (ECT) Trial – Jury Finds Somatics Failed to Warn of ECT Risks
|
By
Wisner Baum
A jury trial in the case Jeffrey Thelen v. Somatics, LLC (Case No. 8:20-cv-01724) took place in May and June of 2023 over the course of seven days before Judge Thomas Barber, U.S. District Court for the Middle District of Florida, Tampa Division. To our knowledge, this was the first case involving severe personal injury allegations against an electroconvulsive therapy (ECT) device manufacturer to proceed to trial.
Electroconvulsive therapy, often referred to as “shock treatment,” is used for treating severe depression and bipolar disorder by applying a brief intense electrical current to the patient’s head to induce a grand mal seizure.
Plaintiff Jeffrey Thelen alleged in his lawsuit that Somatics failed to adequately warn about the known risks associated with its ECT machines, including brain damage, severe permanent memory loss, permanent neurocognitive injuries, and others.
After seven days of trial proceedings, the jury in Jeffrey Thelen v. Somatics, LLC found that Somatics failed to warn about the risks associated with its ECT devices. However, the jury concluded that this failure was not a proximate (i.e., legal) cause of Mr. Thelen’s injuries. Thelen has filed a motion for a new trial arguing that, because his design defect claim was dismissed; improper instructions were given to the jury; critical evidence was excluded at trial (including a video of the doctor showing he was not fully aware of the risks); and Somatics’ counsel made improper statements in closing argument (misstating the law on proximate cause), Thelen was not given a fair trial and, in the interest of justice, a new trial should be granted.
Plaintiff Jeffrey Thelen, a resident of Nebraska, received 95 electroshock treatments between 2014 and 2016. The ECT machine used to administer electroshock to Thelen during his ECT procedures was the Somatics Thymatron System IV ECT machine.
Mr. Thelen filed a lawsuit in 2020 against Somatics, a Florida-based manufacturer of ECT devices, alleging Strict Liability (Failure to Warn) and Negligence. Somatics denied it was negligent and further denied that the ECT machine was defective as labeled.
During trial, Mr. Thelen’s treating psychologist, who independently performed neuropsychological testing on him, testified that Thelen’s symptoms went well beyond what you would typically see in a psychiatric patient and are indicative of someone who has suffered a brain injury.
Evidence was presented showing Mr. Thelen must carry a pocket notebook to write down basic information so he does not forget it. His home is labeled with descriptions of where items like clothing and cooking supplies are stored to save him hours of his day searching for everyday items. Mr. Thelen’s family and his doctors testified that Thelen often finds himself lost in his own neighborhood, on the way to his parents’ home, and in large parking lots or grocery stores. Testimony presented at trial also demonstrated Mr. Thelen lost key autobiographical memories, including forgetting precious childhood memories, his cousins and extended family, and even his ex-wife.
Thelen Trial Transcripts
Redactions were made of side bars and certain sensitive personal information.
Thelen v. Somatics Trial
“But for me, studying the central nervous system was its own reward. The brain was a magic mushroom, two plus pounds of electrical jelly, the circuitry of consciousness … I was teased by the notion that the brain is more quintessentially ‘self’ than any other part of the human anatomy … And I came to conceive of the neurologist as a protector of the brain, not only from bacteria, viruses and trauma, but from overly ambitious fellow creatures—especially those who would harm the brain to help mankind, that is the practitioners and proponents of electroconvulsive therapy.” Quote from the American Psychiatric Association Task Force Report, 1978, p. 135.
Opening Statement for Plaintiff by Bijan Esfandiari
Opening Statement for Defense by Susan Cole
Plaintiff’s Expert Witness, Dr. John Read - Direct Examination by Bijan Esfandiari
Dr. John Read is a Professor of Clinical Psychology at the University of East London in England. He has an undergraduate degree in Psychology and a master’s degree and Ph.D. in Clinical Psychology. Dr. Read has written over 200 peer-reviewed medical journal articles as well as written and edited five books and contributed over 50 book chapters, several of which include discussions of ECT, its lack of efficacy and ability to cause brain damage.
Read Key Testimony
Dr. Read reviewed all studies that have ever been conducted that compared ECT with “sham” ECT. This is the gold standard way to determine if a medical treatment works, it is widely accepted, and constitutes evidence-based medicine.
Only 11 such studies exist, all predating 1986. These studies would not pass muster today – they were of very poor quality.
“We can say there has never been a single study showing that ECT is better than sham ECT beyond the end of treatment, or ECT cannot be said to have any long-term benefits.”
With respect to brain damage, Dr. Read testified “several leading proponents [of ECT in earlier times] argued that ECT works because it reduces the intelligence or level of intellectual functioning of people. So they were arguing that some mental patients have too much intelligence, too much going on in their brains, and it needs to be reduced, and they believed that that was the therapeutic process.”
“The other type of brain damage they said was helpful was that it erased traumatic memories. So if people had upsetting memories from the past, it was a good idea to erase them with electricity. So this idea was generally thought about as what they called brain-damaging therapeutics [a theory that included lobotomies], which is strange looking back, but at the time, that was a genuinely held belief.”
“[W]e have published a review of over a hundred studies to support this idea, is it’s similar to the original brain-damaging therapeutics idea, and we have, we believe, demonstrated that the effects on the brain that the ECT is very similar to the effects of what’s called a closed-brain injury … there’s changes in the brain that are documented after ECT, very similar to traumatic brain injury.”
With respect to permanent memory loss, Dr. Read testified “our analysis indicates that the range of a percentage of the people who get autobiographical memory loss is between 12 percent and 55 percent” and “[t]his is permanent memory loss.”
Transcript of April 29, 2021 deposition of Dr. Richard Abrams
Examination by Plaintiff’s counsel, David Karen; Somatics’ counsel, David Poole; and Bijan Esfandiari
Richard Abrams M.D. is co-owner of Somatics LLC with Dr. Conrad Swartz.
Abrams Key Testimony
Q. Let me ask you, as the manufacturer of the Somatics machine, have you or your company taken any efforts to conduct a clinical trial that you believe in your mind, would answer the question of whether ECT can cause either brain damage or permanent memory loss?
A. No.
Q. And Somatics has likewise never conducted any clinical trials to determine the safety and efficacy of its ECT machines, correct?
A. It has not. Correct.
***
Q. At any time to the present, has Somatics initiated any studies or tests with regard to this issue of long-term side effects associated with ECT?
A. No.
Q. Any reason why not?
A. That’s not our business.
***
Q. Up to this point in time, had you reached any conclusions as to how ECT was working in terms of its effectiveness?
A. No.
***
Q. Up to the present, do you have any understanding as to the mechanics of how ECT works?
A. I do not.
***
Q. … would you agree that that’s the general state of the industry still today, that the practitioners of ECT don’t have any understanding of how it works?
A. That’s correct.
***
Q. … do you have any understanding that anyone at Somatics has ever incorporated studies of traumatic brain injury with ECT in any way?
A. Certainly not.
Q. Do you know why?
A. There would be no reason to.
Q. Is that because you don’t believe that there could be a correlation between TBI, traumatic brain injury, and ECT?
A. Well, we’re not in the business of doing studies of traumatic brain injury. We sell Thymatrons.
***
Q. Has Somatics [ ] conducted any studies to determine whether any brain injury could be caused by ECT?
A. Somatics has never conducted any studies of any kind.
***
Q. [In 1978, ECT proponent, Dr. Max Fink wrote] Quote, the principal complications of EST [Electroshock Therapy], or ECT, are death, brain damage, memory impairment, and spontaneous seizures. These complications are similar to head trauma to which EST has been compared.
A. I disagree.
***
Q. In terms of your first exposure to ECT, was there a measurement of time associated with inducing seizure that you had adopted as necessary to promote the therapeutic effects you were seeking with ECT?
A. It was a rule of thumb that was not based on any specific evidence in the literature, and that was it should last at least 30 seconds … It was just a clinical rule of thumb.
Q. And do you know where that rule of thumb came from?
A. Plucked it out of the air, as far as I know …
***
Q. … Fair to say from that point in time to the present, there has always been – that you’re aware of – complaints that permanent long term memory loss is a risk associated with ECT?
A. Correct.
Q. Fair to say that you just disagree with it?
A. I do.
***
In reference to a quote from Peter Sterling, a neuroscientist from the University of Pennsylvania, who wrote: “One can be sympathetic to psychiatry as I am and still imagine that passing 150 volts between the temples to evoke a grand mal seizure might cause brain damage. Especially, when you realize that this cure for depression, cure in quotes, requires this procedure to be repeated 10 to 20 times over a week or so. And when you talk to a friend who has been so treated and discover that a year later, she is still experiencing huge gaps in recall of major life events, you begin to worry. Finally, you discover that ECT's benefit is only temporary, so that many psychiatrists administer it chronically.”
Abrams responded:
Q. … is it also true that Dr. Sterling is not alone in his comments and opinions that ECT can cause brain injury and permanent memory loss?
A. He is not alone.
***
Co-owner Dr. Conrad Swartz wrote in an email “the goals of the warning statement we need to make [re permanent memory loss and brain damage] are one, to prevent lawsuits, and two, not alienate psychiatrists.”
Q. Do you see that doctor?
A. Yes.
Q. Do you agree with the statements made by Dr. Swartz? …
A. I would say those are accurate. I would agree with those.
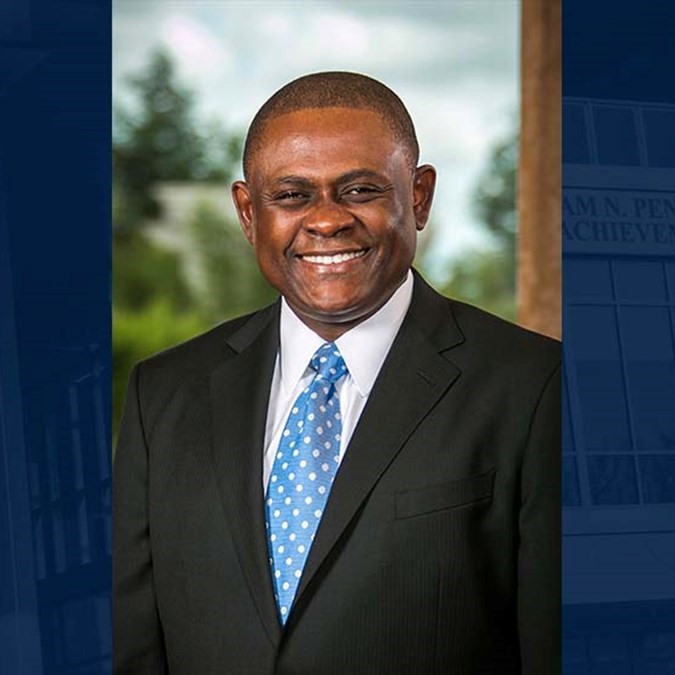
Plaintiff’s expert witness Dr. Bennet Omalu - Direct Examination by Bijan Esfandiari
Cross-examination by Susan Cole
Redirect Examination by Bijan Esfandiari
Dr. Bennet Omalu is a forensic pathologist and neuropathologist. He is a clinical professor of laboratory medicine and medical pathology at the University of California at Davis. He has board certifications in anatomic pathology, clinical pathology, forensic pathology, neuropathology, and medical management, and a master’s in public health.
Dr. Omalu Key Testimony
“A seizure is not a normal event in the human brain … As a normal human being, you should not have a seizure ever in your life. So a seizure being abnormal is a symptom manifesting brain injury, manifesting brain damage … Brain damage could be congenital … or it may be caused by external factors, external energy being transmitted to the brain, be it kinetic energy, chemical energy, or electrical energy. So whenever any human being suffers a seizure, it is a manifestation of brain injury and brain damage.”
“[P]rior to his ECT, I did not encounter or suspect that [Jeffrey Thelen] had any significant memory impairment. His memory was intact.” After receiving 95 ECT treatments, Jeffrey Thelen “has permanent and severe memory impairment.” Mr. Thelen’s multiple ECT treatments were “a substantial and significant factor that caused his brain damage.”
Plaintiff’s expert witness Kenneth Castleman - Direct Examination by Bijan Esfandiari
Cross-examination by Susan Cole
Redirect Examination by Bijan Esfandiari
Kenneth Castleman is a biomedical engineer with a Master of Science degree in electrical engineering, and a Ph.D. in biomedical engineering from the University of Texas at Austin. Professor at CalTech, Pasadena, California. He worked with NASA for 15 years and has done research on the electrical mechanics of ECT and its impact on the human body and brain.
Castleman Key Testimony
Q. So in Mr. Thelen's ECT treatment, he had 3 billion billion electrons of energy transmitted out of this machine, correct?
A. 3 billion billion electrons, yes, forced through his head, correct.
Q. … The 3 billion billion electrons that are being transmitted, is that a lot of current?
A. It is relative to what a human body is accustomed to seeing. Yes, it is a lot of current.
Q. So in terms of -- if you -- you mentioned 3 billion billion electrons in one amp is a significant amount of current. I'm asking you can you please compare that to another product that we, the jury, or the people in this courtroom may be familiar with? …
A. Such as a taser, for example, can incapacitate a person in about a second using 3.6 milliamperes of current, average current. The Thymatron uses 900 milliamps in its pulses, and if you take into account the dead time between the pulses, the average current is about 63 milliamps, so -- over an 8-second period. So the taser gives the suspect 3.6 milliamps for one second average current, and the Thymatron gives the patient 63 milliamps of current for 8 seconds …
[T]he average current delivered by the Thymatron for 8 seconds is 16 times the average current delivered by a taser for one second.
On cross-examination, Somatics’ counsel attempted to downplay the number of electrons flowing through an ECT patient’s head by comparing electrons in water.
Q. So the number of electrons in a quarter of a teaspoon of water from the hydrogen alone, not counting the oxygen in the water, but just from the hydrogen alone is -- well, a whole lot more than a billion billion?
A. That's correct.
Q. So when you're talking about 6 billion -- when you're talking about 1 billion billion electrons going through a current, that sort of puts it into perspective; doesn't it, sir?
A. No, not at all –
Q. I see.
A. -- because what we're talking about here is electrons moving. As long as those electrons are sitting still, it doesn't create any –
MS. COLE: Your Honor, I asked him a yes/no question.
THE COURT: Yes. His answer was yes or no?
THE WITNESS: I'm sorry. Repeat, please.
THE COURT: Ask the question again. Answer yes or no, please.
MS. COLE: Could the reporter please repeat back my question?
THE COURT: So the number of electrons in a quarter of a teaspoon of water from the hydrogen alone, not counting the oxygen in the water, but just from the hydrogen alone, well, is a whole lot more than a billion –
MS. COLE: I think I said billion billion.
THE COURT: Billion billion.
THE WITNESS: Yes, if I understand your question correctly, the number of electrons in a gram of water, the hydrogen alone is more than 6 billion billion.
On redirect, Plaintiff’s counsel asked Dr. Castleman:
Q. Now, there [were] a few questions she asked you that you wanted to explain further. I frankly couldn't understand her questions. She was talking about how many electrons are in water versus the electricity that this machine is generating to cause a seizure. You began to explain, but then you were prevented from doing so. Please go ahead and give us why the analogy she was talking about when it came to water versus electricity, why that is not an accurate analogy.
A. Okay. The point she was making is that there are a huge amount -- huge numbers of electrons in everything. Even a small amount of water has billions and billions of electrons in it. But when we talk about current, we're talking about the number of electrons that are moving, because if an electron is just sitting there spinning around its nucleus, no heat is generated. No harm is done. But once those electrons start moving, that's when you get energy transfer, when you get heating building up and other changes taking place in the tissue.
So the thing that's important in this situation is the current, the movement of the electrons, and so what we're concerned with here is how many electrons are moving during the treatment. That's what determines the amount of the dose.
Q. And that's why when we drink a cup of water, we don't get a seizure, right?
A. Correct. Those electrons are not causing any trouble.
Q. Right. And that's why when we drink a cup of water, nobody need put us under anesthesia and give us muscle relaxers, right?
MS. COLE: Objection, Your Honor. Beyond the scope.
Defendant witness and co-owner of Somatics, Dr. Conrad Swartz - Direct Examination by Jason Benkner
Cross-examination by Bijan Esfandiari
Redirect Examination by Jason Benkner
Dr. Conrad Swartz is co-owner of defendant Somatics LLC, with Dr. Richard Abrams, and designed the Thymatron ECT device. Prior to designing Somatics’ ECT device, Dr. Swartz regularly performed ECT procedures on patients.
Conrad Swartz Key Testimony
On direct examination by Somatics’ counsel, Dr. Swartz testified:
Q. … Doctor, are you concerned at all about the amount of electricity that's put out by ECT devices?
No, I am not. It is not much.
Q. … When you were a practicing psychiatrist, did you ever review the scientific and medical literature on ECT to stay current on what's happening in the field?
A. Yes. To stay current and also to teach the students and the residents with accurate current information and also to improve the quality of the ongoing research studies that I was trying to do.
On cross-examination by Plaintiff’s counsel, Dr. Swartz testified:
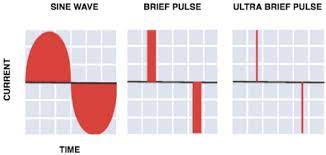
Q. … Does ECT, whether used in sine wave or ultra pulse or Thymatron machine, does it cause brain damage?
A. It is not known to cause brain damage. There's no evidence for it, and I have not seen that.
Q. All right. So are you -- when you formed Somatics and put out your first Thymatron machine, were you familiar with the literature that preceded you?
A. Yes.
Q. Did you rely on that literature in ensuring that your product is going to be safe and effective?
A. Yes.
***
Q. Let me go through some of that literature. Were you familiar with a paper by Alpers, called "The Brain Changes and Electrically Induced Convulsions in the Human"?
A. I don't recall this particular one.
Q. … Were you aware that Dr. Alpers published a number of publications inquiring whether ECT causes brain damage?
A. I don't recall.
Q. The conclusions of this paper -- these were biopsies that were done on individuals who had recently died after convulsive therapy. Are you familiar with the literature that analyzed the brain tissue of dead people after ECT?
A. I have seen at least some of that literature.
Q. And you agree with me that some of that literature actually found what they attributed to be brain damage caused by ECT?
I believe they claim that.
***
Q. So let's look at this paper and its conclusion writes. "Those observations showed the damage to the brain, sometimes reversible but often irreversible, occurred in the course of electric shock treatment." Were you aware of these findings when you put out your Thymatron machine into the public?
A. I was aware that such reports had appeared in the old literature. Not this specific report.
***
Q. Are you familiar with a paper by Goldman from 1972?
A. I wouldn't say familiar. Maybe I had seen it.
Q. All right. This paper, "Long-term Effects of Electroconvulsive Therapy upon Memory and Perceptual Motor Performance," does this refresh your recollection, if you recall this paper?
A. I don't recall it.
Q. In this study, this was not an autopsy report, but they were -- in looking into people who had received more than 50 ECT treatments to determine what impact it had on their cognition. Were you aware that such a study had occurred?
A. Nope.
***
Q. Let's look at the findings, Doctor … So it states, "The significantly greater error scores obtained by ECT subjects on both the Bender-Gestalt and the Benton," those are memory tests, "after a relatively long time period since the last course of treatment suggests that ECT causes irreversible brain damage."
Were you aware of that?
Nope.
***
Q. How about this paper from 1973 by Templer, "Cognitive Functioning and Degree of Psychosis in Schizophrenics Given Electroconvulsive Therapy"?
Are you familiar with this publication, Doctor?
No.
Q. In Templer, they were trying to test the conclusions from the prior article that I showed you, the Goldman article. Let's look at their findings. The ECT patients' inferior Bender-Gestalt performance does suggest that ECT causes permanent brain damage. Were you familiar with that, Doctor?
A. No.
Q. Putting in front of you what we're identifying as the article by John Friedberg, "Shock Treatment, Brain Damage, and Memory Loss: A Neurological Perspective." This was published in the American Journal of Psychiatry in 1977. Are you familiar with this paper, Doctor?
A. No.
Q. This paper, they were looking into the issue of ECT and brain damage. I want to look at the conclusions here. It states, "Many psychiatrists are unaware that ECT causes brain damage and memory loss because numerous authorities and leading psychiatric textbooks deny these -- deny those facts." Do you see that, Doctor?
A. I see it in front of me.
Q. When you -- since 1977, this is about eight years before you formed Somatics. Correct?
A. Yeah.
Q. And so you were one of the group of psychiatrists who apparently were unaware that ECT causes brain damage. Correct?
A. I was among a group of psychiatrists who understood that ECT does not cause brain damage, that there's no evidence that ECT causes brain damage.
***
Q. Are you familiar with this publication from 1978, sorry, comprehensive -- the journal is Comprehensive Psychiatry, titled, "Efficacy and Safety of Induced Seizures in Man" by Max Fink?
A. I don't remember this article.
Q. Drawing your attention to a section of this paper entitled safety. I'm going to start reading from right here. "The principal complications of EST" -- and EST is ECT. Correct, Doctor?
A. Yes.
Q. It used to be called electroshock therapy back then. Correct?
A. Yeah.
Q. But it's still the same electroconvulsive therapy?
A. Yeah.
Q. It states, "The principal complications of EST are death, brain damage, memory impairment, and spontaneous seizures." Did I read that correctly, Doctor?
A. Yes, you did.
Q. Were you aware of that when you put out your Thymatron machine?
A. I was aware of his statement.
Q. You were aware of his statement?
A. Yeah.
***
Q. … and the literature continued to look into the issue of whether ECT causes memory loss and brain damage. Do you agree with me, Doctor?
Yes.
***
Q. Is it possible to have cellular damage and it not appearing on an MRI machine?
I believe so.
***
Q. Assume -- we have your ECT in the other room, but I don't need to bring it out. If we brought it out here and applied it to me with no anesthesia or anything, what would happen when you hit the on button?
It would knock you unconscious.
***
Q. Have you read literature to suggest when ECT is administered it causes brain cells to die?
No.
Q. Okay. Let's look at study here from Neuroscience and Behavioral Psychology in 2005. Apologies. "Electroconvulsive Shock Induces Neuron Death in the Mouse Hippocampus: Correlation of Neurodegeneration with Convulsive Activity." Are you familiar with this study, Doctor?
A. No.
Q. Let's take a look at the conclusion. The data reported here support the concept that significant functional changes following repeated electric shocks do occur. They deepen our understanding of this phenomenon by providing direct evidence for a moderate, up to 10 percent, but significant level of neuron death in particular parts of the hippocampus due to shocks. Were you familiar with that study, Doctor?
No.
***
Q. And do you believe you have a responsibility to continue to review the literature and the science that it develops to continuously update your manual and ensure that the most recent data is made available and published in your manual?
A. Yes.
Q. Are you familiar with a study done by a Dr. Sackeim from Columbia University in 2007 titled, "Cognitive Effects of Electroconvulsive Therapy in Community Setting"?
A. I have read this paper several times …
***
Q. Okay. You agree with me that his study found that 12.4 percent of the patients had marked and persistent retrograde -- we'll just read it together. Of the 306 patients classified, 12.4 percent patients met the a priori criteria for having marked and persistent retrograde amnesia on the AMI – I believe that is the autobiographical memory inquiry. Do you see that, Doctor?
A. I see it. I dispute it.
***
Q. And because you don't agree with it, you never updated your manual to warn about the findings from the Sackeim paper. True?
A. We did not change what was in the manual in response to what Dr. Sackheim wrote.
Q. Yeah. We both agree that your manual makes no reference to brain damage, correct …?
A. The words do not appear in that -- explicitly in that manual.
Q. You -- your manual … makes reference to the APA Task Force. Correct?
A. Yeah.
Q. And it encourages psychiatrists to read this from 2001. Correct?
A. It directs them to read it.
Q. …. I represent to you that this is a page from the same APA. Does this look familiar to you, Doctor?
A. … I am familiar with the meaning of this statement.
Q. Okay. And I can try to see. What does it say in the part that I've highlighted, Doctor?
A. In light of the accumulated body of data dealing with the structural effects of -- structural effects of ECT … brain damage … should not be included as a potential risk of treatment.
Q. So this tells doctors don't warn about brain damage. Right?
A. That's what it says.
Q. And you told doctors to go read this. Right? And to rely on this and make their -- the information that they give to patients to be based upon this book and a doctor reading this book, according to your instructions, then is told do not warn patients about brain damage. Right?
So he's told.
***
Q. … Showing you, Doctor, it's an e-mail from you to a Holly -- psychiatrist named Holly Lisanby. Do you know that individual?
A. Yes.
Q. Is this your e-mail address, Doctor?
A. Yeah.
Q. And you were letting her know that you were interested in a book proposal. Do you see that, Doctor?
A. Yes.
Q. And you're discussing competing publications. Can you please read for me -- and you said the competing publications are Dr. Abrams' book, who is your partner. Correct?
A. Yes.
Q. And the other competing publication is the APA Task Force. Correct?
A. Yes.
Q. Can you please read into the record your comments about the APA Task Force?
A. … "The other book is American Psychiatric Press APA Task Force Report 2001, quote, the practice of electroconvulsive therapy, period, recommendations for treatment, training, and privileging, period, second edition, period, closed quote. "It has 243 large-print pages plus references. This book is psychiatrist centered and apparently aims to make permissible as much as possible. This is what a task force should do. To illustrate the extremity this has taken, the book section on patient selection figuratively throws up its hands about which patients with major depression should or
should not receive ECT. "It is a book of administrative policy that withholds basic judgments, including clinical advice about what works best. This book probably decreases litigation risks because virtually everything is permissible. Although this is nice for clinicians, it provides virtually no guidance for how to practice."
Q. Still think this is the most authoritative book on ECT?
A. Yeah.
***
Q. You … made some reference to the sine wave, the old sine wave machines being more dangerous than the current machine that you're manufacturing.
A. Yes.
Q. … You have a book published out currently. Correct, Doctor?
A. Yes.
Q. That Electroconvulsive and Neuromodulation Therapies?
A. Yes.
Q. Okay. Let's go to the preface. I'm sorry. Let's go to -- Chapter 1 of your book is an article titled, "Electricity and Electroconvulsive Therapy" by Conrad Swartz?
A. Yeah.
Q. … The section here, "Sine Wave Versus Brief Pulse Stimuli." Since these are your own words, I'll let you read them please.
A. "The report that brief pulse stimuli have milder side effects and use less charge than sine wave stimuli do is well known. However, the result was never proven as just stated.
Q. And am I understanding you correctly, do you believe that the hippocampus is injured at all as a result of ECT?
A. No. Based on recent studies.
Q. And in this book of yours we've been talking about, when was it published, Doctor?
A. 2009, as I recall.
Q. And I'm looking at the preface, you wrote the preface?
A. Yes.
Q. Can you read for me what I've highlighted there, Doctor?
A. "The numerous alterations in the hippocampus with ECT suggest its involvement in ECT mechanism, but this part of the brain is particularly given to change. This tendency to change, together with its involvement in memory, suggests that the hippocampus may be involved in ECT cognitive effects, side effects, as well as efficacy."
Q. You believe that to be true still today?
A. Yeah.
Q. Yes?
A. Yes.
Q. So why is it when I asked you if ECT is associated with damaging the hippocampus, you said no?
It's not damage. It's alterations.
***
Q. In your book, you state, "Several reports from Columbia University claim that medication-resistant major depression responds poorly to ECT," and cites publications. True?
A. Yes. Prudic is a coauthor of Sackeim. Sackeim is a coauthor of studies of Prudic, yes.
Q. This information was nowhere in your manual. Correct?
A. Correct.
***
Q. But just so we're clear, your testimony is that the cells in the hippocampus are impacted by the ECT machine, but whatever impact that has in -- your testimony is that it's positive?
A. By the ECT treatment, not the ECT machine. And it's positive, yes … It’s positive and temporary.
***
Q. And you recall, though, we did see some literature, including something from your own book, where it mentioned that that is also the reason for the cognitive decline that some people may experience. True?
Not decline. Cognitive temporary impairment.
***
Q. All right. Well, let me ask you, if -- in deciding what warnings to give to doctors, you agree with me that when you were writing your manual, the manual that's in effect in this case, the 2013 manual, that, at that time, there was a debate, which remains to this day, as to whether or not ECT causes brain damage. True?
A. Not true. I don't agree.
Q. No. So all those literature that we looked at that made reference to brain damage, the experts that this jury has heard from that talked about brain damage, the discussions in the books that you yourself wrote, and so forth, none of those, in your opinion, is -- are indicative of even a debate existing?
A. Correct. Well, they're indicative of a disagreement. Disagreement doesn't mean there's debate.
Q. Okay. And you -- because you draft the manual, you get to be the arbiter and the judge of who wins that debate, because you're the one who decides what are you going to warn in your manual. True?
Okay.
Q. And as a result of your decision, whoever reads your manual is not going to be warned about brain damage or dementia. True?
A. Is not going to be warned by this manual of that. They can find other sources that say other things …
But I can assure you that what's in the manufacturer's literature is not the latest understanding or the best understanding or the most complete understanding. It is a description of what must be said.
Q. Okay. And you and Dr. Abrams chose not to include any warnings about brain damage in the 2013 manual. True?
True.
***
Q. … Are you familiar with a study done by Dr. Calloway, even as early as 1981, that found structural brain changes in ECT patients?
A. I can't place it.
Q. Let me help you out … This is Dr. Calloway, 1981, titled "ECT and Cerebral Atrophy. A Computed Tomographic Study," CT study. Correct?
A. Yes.
Q. Let's go to the discussion. "The result suggests an association between history of treatment with ECT and cortical atrophy in the frontal region." That's the brain. Right, Doctor?
That's part of the brain.
Q. And so -- that's just one study. You can look at others. But you still stand by your statement here that there have not been -- that the side effects are only subjective and have not been related to observable structural brain changes? You still believe that?
A. Yes. You've taken his conclusion out of context.
Q. You've seen other publications that have found structural brain changes after ECT?
A. … I've seen defined structural changes of patients who are selected for ECT where the structural changes occurred before ECT …
***
Q. Okay. All right. Going back to the warning. I want to draw your attention to an e-mail from 2006 between you and Dr. Abrams. Do you remember this, Doctor?
Yep.
Q. All right. Dr. Swartz, this was an e-mail between you and Dr. Abrams concerning the drafting of the disclaimer that we looked at. Correct?
Yeah.
Q. And this is the one you were informing the jury that you thought this was going to be a private discussion not to be shared publicly. Correct?
Yes.
Q. All right. So I want to show you -- draw your attention to a couple parts of this. First, you say, "The goals of the warning statement we need to make are, one, to prevent lawsuits and not alienate psychiatrists." Do you see that, Doctor?
Yes.
Q. You go on to say, "All warnings that are written are stated in the form that this product can or may cause XX. We should conform to this. Cigarette companies cannot use a statement such as nothing in this advertisement should be regarded as a statement that cigarettes do not cause cancer.
This is not a warning." Did I read that correctly?
A. Yes. It's a disclaimer.
Q. So contemporaneous with drafting this disclaimer, it was your belief that it was not a warning. True?
It's what I said in the course of an argument.
Q. And then you go on to say, "Loss of memories is more accurate than memory loss, which smells of dementia. Loss of memories is subjective and does not reflect brain damage." Did I read that correctly?
A. Yes.
Q. Okay. So you wanted to make sure that whatever you were warning about in this disclaimer, that it didn't infer that it's causing dementia, and it didn't infer that it's causing brain damage. True?
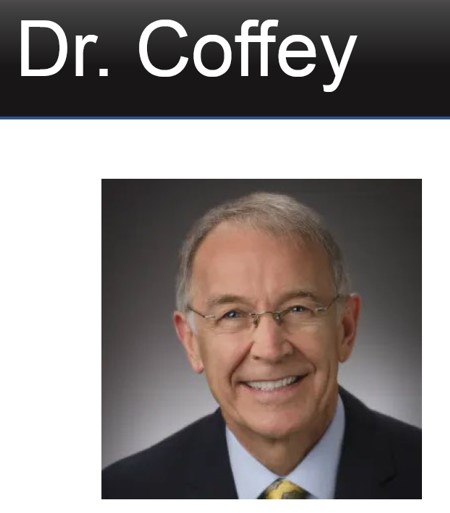
Defense expert witness C. Edward Coffey, M.D. - Direct Examination by Susan Cole
Cross-examination by Bijan Esfandiari
Redirect Examination by Susan Cole
C. Edward Coffey, M.D. is a neuropsychiatrist and was affiliate professor of psychiatry and behavioral sciences at the Medical University of South Carolina in Charleston, South Carolina. He was responsible for creating the ECT program at Duke Medical School. He trained psychiatrists on the ECT procedure and conducted many thousands of ECT treatments at the hospitals where he was employed. He was on the American Psychiatric Association Task Force, that wrote the book “Practice of Electroconvulsive Therapy Recommendations for Treatment, Training, and Privileges,” which includes a recommendation that “brain damage should not be included as potential risk of treatment.”
Dr. Coffey Key Testimony
Dr. Coffey testified, as Somatics’ owners did, that ECT researchers do not know how ECT works:
A. We don't really know how ECT works. Now, we know the seizure is critical. If you don't have the seizure, you don't get better. So something is going on magically with the seizure to bring about the improvement. It is an enduring improvement … So those changes are enduring.
Q. Are those changes -- do those changes cause permanent structural damage to the brain?
A. No. There's no evidence of that.
***
Dr. Coffey was a member of the APA Task Force that wrote the APA ECT Task Force book.
***
Dr. Coffey dismissed patients’ claims of permanent memory loss and the medical literature discussing the same, suggesting it is all in their heads. Dr. Coffey testified:
The major cognitive side effects are on memory. And there are two basic domains of memory that are affected, anterograde memory, the memory
for things that we learn after the ECT and then retrograde memory, memory for events that happened before the treatment … Both, as far as we know, are temporary, short lived, at least as far as we can measure them. And there's no permanent loss of ability to learn and to
remember.
***
The area that remains unclear is the area of retrograde autobiographical memory … those kinds of memories are very, very hard to measure and very hard to quantitate … there are a minority of patients who report that the autobiographical memory remains impaired for extensive periods of time after ECT. Most people don't. Most people report the memory to be improved. But there is a proportion who purport the opposite … And the bottom line here is that it's very, very difficult to find an objective correlate of that complaint.
***
… we acknowledged that, in some cases, the complaints could indicate the loss is permanent. They have not been able to – at least the sensation is that I can’t recover that memory. Again, we don’t have any objective data that that’s the case. But the person certainly feels like that’s the case …
Q. Is that sort of a psychological overlay?
A. Well, certainly, there is a psychology to it. I'm sure that's distressing to the individual. And the problem is that if a person becomes convinced that their memory isn't working and becomes invested in that belief, it could be very, very difficult to change it.
***
Q. The type of memory problem that Mr. Thelen describes, is that something that ECT has the capacity to even do? I don't think so. I'm not sure what else outside of ECT could even do it,
as I mentioned a moment ago. That sort of picture doesn't appear in nature.
Q. What about a psychological overlay. Is that -- can that cause this kind of a syndrome?
A. Well, I guess depends on what you're calling the syndrome. As I said earlier, I don't have any reason to question the sincerity of Mr. Thelen's belief about his memory difficulties. I also believe that he at this point in his life is very invested in this issue. It is, after all, going to trial. And in my clinical experience, once that train sort of leaves the station, it's almost impossible to fix it, to correct it.
Q. Does this feeling of persistent or permanent memory loss mean that the
individual has suffered brain damage?
No. In no way. And we never meant to imply that at all.
***
Dr. Coffey admitted that brain damage would not necessarily show up on a standard MRI or CT scan.
Q. If there were brain damage in an individual, would it show up -- if it were extensive enough to cause this kind of a loss, would it show up on MRI or CT scans?
A. Well, it depends on what the nature of the damage is, how extensive it could be. So the answer could be possibly, but not always …
***
Although the Court had ruled that mention of the FDA would be excluded from the trial, and Somatics’ counsel purportedly instructed him not to discuss it, Dr. Coffey nonetheless testified:
Q. In terms of the issues that we're dealing with in this case, in other words, the risk factors and the possible adverse effects from ECT, is that changing?
No. The basic theme is the same, that is to say that the objective memory side effects are short term and have resolved within a matter of days to a couple of weeks past a completion of the treatment. We still are struggling with this notion of retrograde autobiographical memory. We don't have good information on that even today. Indications have changed a little bit in that the FDA has approved ECT for certain specific indications.
Plaintiff’s counsel explained at sidebar that Dr. Coffey impermissibly said “ECT has been approved by the FDA. Not only is that a violation of the motion in limine, it’s a lie. ECT has not been approved by the FDA.” The Court asked to speak with Dr. Coffey before the jury was brought back in to “tell him what problems he caused for us by doing this.”
The Court admonished Dr. Coffey outside the presence of the jury explaining that his failure to abide by the motion in limine could have serious consequences, including a mistrial and that statements such as the ones he made during his direct examination could “poison the well by bringing up something they weren’t supposed to bring up. That’s what a big deal it is.”
The Court: … You caused some problems for us by talking about the Cuckoo’s Nest and the FDA thing. That’s a big deal to the lawyers. Did your lawyer tell you not to bring that up?
THE WITNESS: Not to bring it up?
THE COURT: Or not -- not even to speak the words. I mean, what were you told?
THE WITNESS: Yes, she did. And I just lost track of it, so it's my bad.
THE COURT: Yeah. There are situations, I don't think this is one of them, but I think you should understand, we've been here since last Wednesday. We've got a jury of eight people who don't get paid. They've got to come and sit here all day and listen to basically somebody else's problem … you blurting -- you mentioning what you mentioned could, in some situations, cause me -- or cause the judge to tell everybody to go home and say the last week of your life that you sat here on jury duty, the week that the lawyers spent here, they're paying several hundred dollars an hour for all these lawyers, it's all gone. Adios. Go home. Because that witness poisoned the well by bringing up something they weren't supposed to bring up. That's what a big deal it is. So it's very important that you listen to what your lawyer tells you, and you do not cross those lines. And if you think you're getting close to maybe needing to cross that line, or you think you need to say that, ask me for a break, and we'll take a break and we'll talk about it. Because that -- that's just the way trials work. All right?
THE WITNESS: Understood.
Plaintiff’s counsel proposed that a curative instruction was necessary and that the jury should be instructed that “the last witness, Dr. Coffey, testified that the FDA has approved ECT. That statement is factually incorrect and should be disregarded by the jury.”
The Court denied Plaintiff’s proposed curative instruction and ultimately instructed the jury as follows: “All right. And, members of the jury, at some point in the last witness’s testimony, a reference was made to the FDA, also known as the Food and Drug Administration. You are instructed that information relating to the FDA has no relevance in this case and should be disregarded. All right?”
***
Cross-examination by Plaintiff’s counsel, Bijan Esfandiari:
Q. [In your report], you stated that none of Mr. Thelen's ECT
providers did anything wrong. True?
I think I -- to that effect, yes, correct, the treatment was performed
appropriately, and there were no adverse complications from the treatment.
Contrary to the evidence, Dr. Coffey testified that no doctor had ever diagnosed Mr. Thelen with a major neurocognitive disorder (characterized by damage to nerve cells in the brain) or dementia (which is caused by damage to brain cells).
Dr. Coffey also testified that Mr. Thelen never articulated to any medical professional that he had lost his memory.
His testimony was effectively proven to be completely false during cross-examination with presentation of clear medical record evidence and prescriptions for dementia drugs. Plaintiff’s counsel used the following demonstrative to illustrate Coffey’s errors:
At one point during his testimony, Dr. Coffey snapped at Plaintiff’s counsel’s cross-examination, complaining “I find that perjorative.” He further lost his cool during the following exchange and was admonished once again by the Court:
Q. Let me ask you, when was the last time an autopsy had been performed on a person who had received ECT?
How would I know the answer to that?
Q. I thought you've been studying ECT for 40 years, that you've written books, we saw a couple of your books, that you authored the APA Task Force book. And your testimony, you came here and told us that ECT doesn't cause brain damage or neurocognitive decline is permanent. And you're telling me that you don't remember the last time somebody did an autopsy of a patient who had ECT?
A. First of all, I find your tone insulting, number one. And, number two, how could I possibly know –
THE COURT: Stop. Stop. Stop. Members of the jury, please retire to the jury room. Thank you.
THE COURT SECURITY OFFICER: All rise for the jury.
THE COURT: This is not a conversation between you and him. Your opinion of his questions being pejorative or insulting is not relevant evidence in a case.
THE WITNESS: Yes, sir.
THE COURT: All right. You've already done two things. You've said something about the FDA, which was against what your lawyer said to do, and you did another thing, which escapes me now. All right? I'm trying to get you out of here to make your plane. I'm not sure that's going to happen if this continues …
THE WITNESS: Okay.
***
In contrast to Dr. Bennet Omalu, Dr. Coffey admitted he is not an expert concerning brain injury:
Q. And do you consider yourself as an expert on the issue of brain injury?
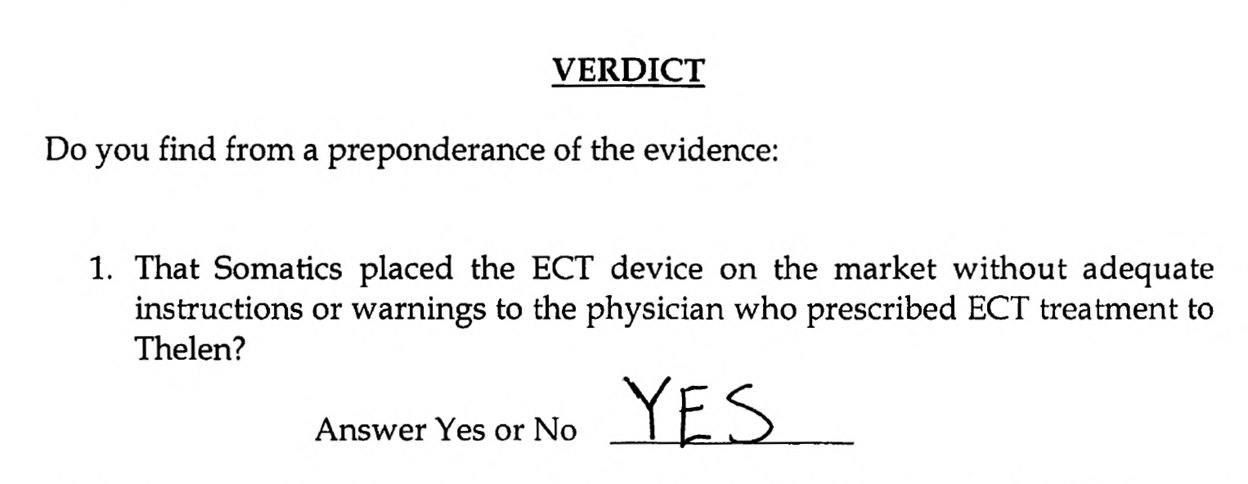
Verdict: Jury unanimously finds that Somatics placed the ECT device on the market without adequate instructions or warnings to the physician who prescribed ECT treatment to Plaintiff.
However, the jury finds the absence of adequate instructions or warnings was not a proximate (or legal) cause of Plaintiff’s injury.
Motion for New Trial
On July 7, 2023, Plaintiff filed a motion for a new trial citing several errors justifying a new trial, including that his claim for design defect was dismissed, key evidence was improperly excluded, erroneous instructions were given to the jury, and defense counsel made improper statements in closing which misstated the law on proximate cause.
Transcript of April 29, 2021 deposition of Dr. Richard Abrams
Transcript of July 12, 2018 deposition of David Mirkovich, Somatics General Manager and responsible for selling and promoting the Thymatron ECT device to hospitals and physicians.
Video deposition on June 17, 2022 of Jesse Pavel, President of Elektrika. He supervised Elektrika’s technicians who built Somatics’ Thymatron ECT device and was solely responsible for complying with regulations applicable to manufacturing the device.
Transcript of June 17, 2022 deposition of Jesse Pavel
Transcript of August 10, 2018 deposition of Dr. Conrad Swartz, co-owner of Somatics
Transcript of April 1, 2021 deposition of Dr. Conrad Swartz
Transcript of June 14, 2022 deposition of Dr. Conrad Swartz





 Dr. John Read - Cross-examination by defense, Jason Benkner
Dr. John Read - Cross-examination by defense, Jason Benkner